
In 2020, Nabunya, found joy amid the uncertainty of the Covid-19 lockdown when they welcomed their first child. Despite the hardships of the pandemic; curfews, movement restrictions, and financial strain, the birth of their newborn brought a wave of joy and warmth that lit up their home and helped them endure the tough global crisis.
When the couple decided, after four years, to try for another child, they were filled with hope and anticipation. However, the journey this time proved more difficult, as month after month, Nabunya’s period returned.
This, among other silent struggles, is a heartbreak many women endure in societies where motherhood is not merely celebrated but deeply expected. For Nabunya, each passing cycle felt like both a personal disappointment and a quiet social failure.
“This was the worst news, and knowing that there was no clear medical issue that I had made it even more frustrating. I desperately wanted to conceive, but nothing was happening,” Nabunya recalls.
Dr Charles Lwanga, a gynaecologist based in Luweero, says experiencing difficulties conceiving again after previously giving birth successfully is a common condition known as secondary infertility.
Secondary infertility is usually caused by several factors, including age-related changes that affect egg quality, hormonal imbalances, complications or scar tissue from previous deliveries or surgeries, untreated infections, and conditions such as polycystic ovary syndrome (PCOS).
He notes that while the causes are not always clearly identifiable, seeking medical evaluation is vital to rule out issues such as hormonal imbalances, uterine complications, fallopian tube blockages, or lifestyle-related factors. Early assessment can help determine the right course of action.
After several months of clinging to hope, Nabunya’s prayers were finally answered; she was able to conceive again. During her first antenatal visit, she met with an obstetrician who reassured her that, despite having delivered her first child through cesarean section, she could still aim for a normal delivery this time.
Although she had hoped the same obstetrician would guide her throughout the pregnancy, Nabunya was disheartened to learn during her second hospital visit that the doctor had retired. She came to terms with the change and found comfort in placing her trust in a new obstetrician.
Losing a uterus
At 36 weeks, Nabunya was told that her amniotic fluid levels had significantly dropped, an alarming development, especially given her history of a cesarean section.
Dr Lwanga explains that during sonography, when a physician detects reduced amniotic fluid, a condition known as oligohydramnios, it signals potential risks to both the baby and the mother. In such cases, early delivery, sometimes through a planned cesarean section, is often recommended to avoid complications such as faetal distress or cord compression.
When the doctor recommended another C-section, Nabunya decided to return to her previous doctor, who was more familiar with her medical history, to perform the surgery.
“We made an appointment for the elective cesarean section on August 16, 2024, at 9am. I reached the hospital at 7am to prepare for the surgery and was put on a drip until 5pm when I was taken to the theatre,” she recounts. “When I saw my newborn, I was so delighted to know that she was safe. However, in my mind, I wondered how easily this had happened.”
About an hour after being wheeled back to her ward, while scrolling through congratulatory messages on her phone, Nabunya began to feel a sharp, growing pain deep within her abdomen.
The midwife on duty responded promptly, reassuring her that such discomfort was normal and likely a result of the procedure’s after-effects, especially so soon after surgery.
A few minutes later, the pain intensified and became unbearable. Nabunya asked her sister to call the doctor, only to learn that the one who had performed her surgery had handed over to another on-duty physician. The new doctor arrived, accompanied by three others. After briefly massaging her abdomen, they instructed the midwife to continue monitoring her condition.
Although she experienced brief relief, the pain soon returned, sharper and more intense than before. When the medical team responded again, they massaged her abdomen to ensure the uterus contracted, a routine intervention aimed at preventing postpartum haemorrhage.
Postpartum haemorrhage is a serious condition involving excessive bleeding after childbirth, where a woman can lose between 500 to 1,000 millilitres of blood or more. If not managed promptly, it leads to severe complications or even death.
For Nabunya, the situation took a turn for the worse. Instead of relief, her blood flow increased, and the pain intensified. In response, the midwife administered a drug through the IV drip, but rather than alleviating her symptoms, it caused her to lose her breath.
“I was fighting for my life,” Nabunya recalls. “I could hardly catch my breath and was desperately trying to tell the doctors that I could not breathe. The doctors quickly put me on oxygen and a monitoring machine and told my husband and sister to step outside. They were asked to sign consent forms for another surgery before I was rushed back to the theatre,” she adds.
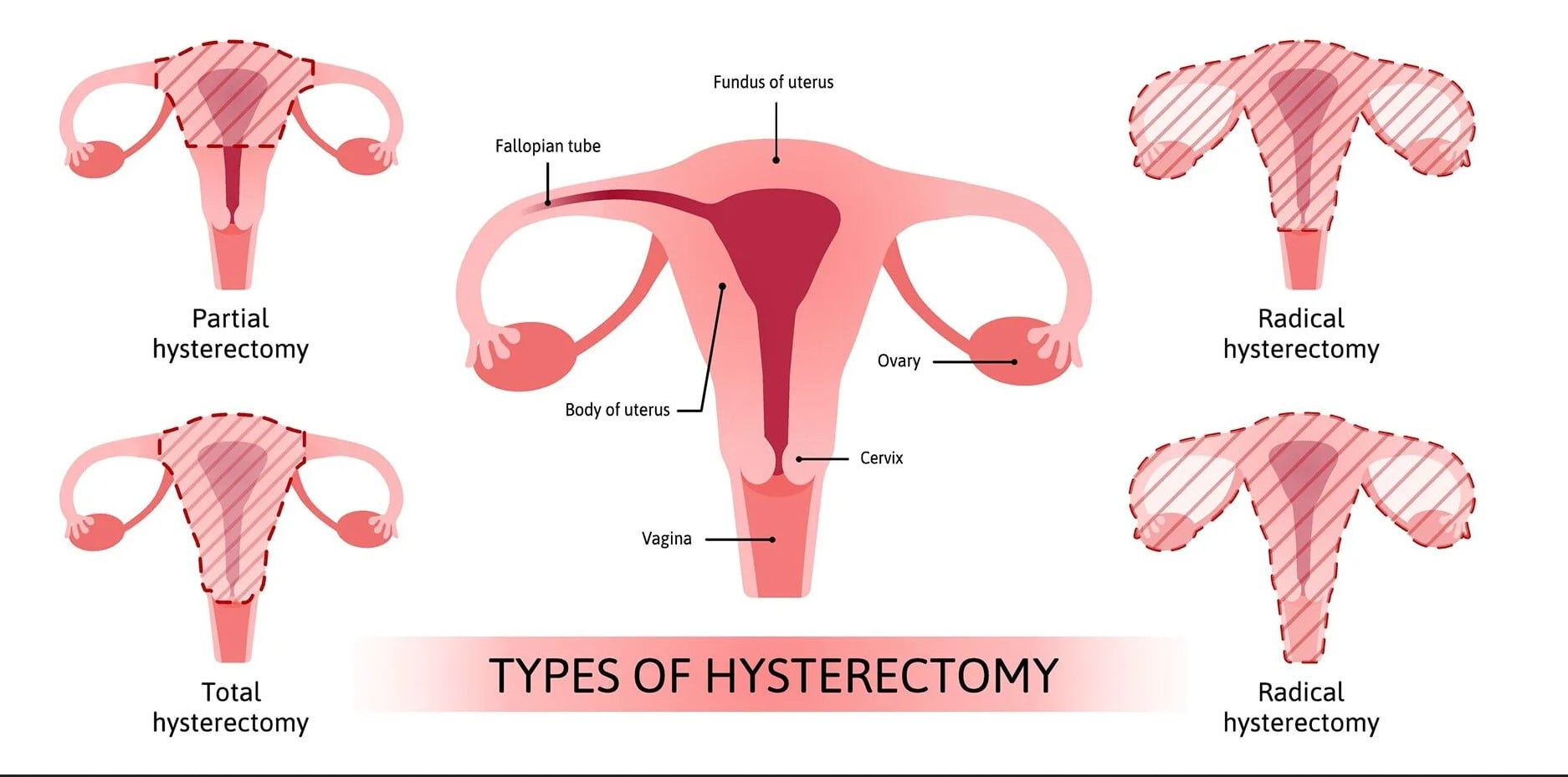
After several hours in surgery, Nabunya was eventually returned to her ward. When she regained consciousness, the doctors conducted a series of checks before gently breaking the news: her uterus had been removed in a partial hysterectomy. They explained that it had been the only option to save her life.
“In my mind, I was not so shocked because I was thankful to God that I was still alive. After four days, I was discharged and went back home, heartbroken, but accepting whatever had happened and ready to start a new chapter of my life without my uterus,” she recounts.
Postpartum mental struggles
Often, when a patient undergoes a life-altering medical procedure, especially one involving loss, such as a hysterectomy, or faces a near-death experience, it is standard practice for doctors to recommend psychosocial support. However, in Nabunya’s case, she was simply discharged with a “get well soon” message from the medical team, without any guidance on emotional or psychological recovery.
While everything seemed normal in the first two months following her surgery, one evening, as Nabunya sat at home with her children waiting for her husband to return, she suddenly felt her heart pause, then restart with an alarming, rapid beat. Alarmed and struggling to breathe, she was rushed to the hospital.
Over three weeks, she underwent a series of tests at different medical facilities to uncover the cause. These included screenings for cardiomyopathy, an echocardiogram, D-dimer test, endoscopy, complete blood count, and checks for pulmonary embolism. Yet, to her confusion and frustration, all the results came back normal.
“I was back home, but with almost no understanding of what was happening to me. The best hospitals in the country had failed to identify the cause of my sudden, on-and-off episodes of breathlessness. Each time it happened, I felt like I was slipping into unconsciousness, and the fear that I might not make it through the next one haunted me constantly,” she says.
Like in many traditional communities, when medical professionals failed to pinpoint the cause of Nabunya’s condition, her family and friends turned to cultural beliefs. Some concluded her suffering was spiritual, possibly a result of witchcraft. They began sharing contacts of pastors and traditional healers, urging her to seek cleansing rituals.
Neighbours recommended natural herbs to bathe in and drink, claiming they would chase away any evil spirits. At one point, a relative even picked her up and took her to a witch doctor; ironically, the healer was unavailable, having gone to seek treatment at a nearby health centre.
Still gasping for breath and growing weaker with each episode, Nabunya remained in distress. While her husband refused to explore traditional remedies, he remained committed to finding a medical explanation. His persistence paid off when a friend referred them to a psychiatrist at Entebbe Regional Hospital, a decision that would finally put a name to Nabunya’s suffering.
She recalled arriving at the hospital still anxious, even asking a nurse if the facility had oxygen. After sharing her history, the psychiatrist diagnosed her with depression, something she initially doubted, wondering how it could cause breathlessness and constant fatigue.
Despite being prescribed antidepressants, she refused to take them until a second visit, when she was diagnosed with panic disorder. With counselling and medication, she began to feel better, remembering her children and regaining purpose. She plans to start a support group for women facing similar struggles and is determined to help others find healing and hope.
Psychiatrist speaks out
Dr Alex Lukwago, a consultant psychiatrist, says postpartum mental health challenges are common, particularly among women who experience traumatic births such as an emergency hysterectomy.
“When a woman gives birth, her body and mind undergo massive changes. For some, especially those who face unexpected complications such as losing the uterus, the emotional impact can be overwhelming,” he says.
The signs of mental health issues during the postpartum period include persistent sadness, unexplained crying, feelings of worthlessness, detachment from the baby, sleep disturbances, loss of appetite, and anxiety.
Dr Lukwago notes, “Some women may begin to experience physical symptoms that resemble heart problems, such as chest tightness, shortness of breath, racing heartbeat, or dizziness, which are manifestations of panic disorder or depression.”
These symptoms are often misdiagnosed in medical settings, especially when a thorough psychiatric evaluation is not part of postnatal care. He highlights that such patients often undergo several expensive tests, blood work, scans, heart checks, only for results to return normal, when the true cause is mental distress.
Recommendations
For mothers experiencing postpartum depression or panic disorder, Dr Lukwago recommends a combination of antidepressant medication, talk therapy, and family support.
“Although counselling helps women process what they have been through, medication can correct chemical imbalances in the brain. Therefore, early intervention is key, and it is vital to always ask for help,” he explains.
Even though stigma around mental health still keeps many women suffering in silence, untreated postpartum mental illness can lead to long-term complications for both mother and child.
He emphasises the need for reforms in maternal healthcare to include mental health screening as part of routine postnatal follow-ups. Hospitals, he says, need to train midwives and doctors to identify mental health red flags.
“Every woman who undergoes major childbirth complications should be referred for psychological evaluation,” he says.
While mental health recovery is a process and involves believing in gradual healing, he encourages women already on treatment to stay consistent with medication, attend therapy sessions, and involve trusted family members in their healing journey, because mental health matters as much as physical healing.
Comments are closed